 |
|
 |
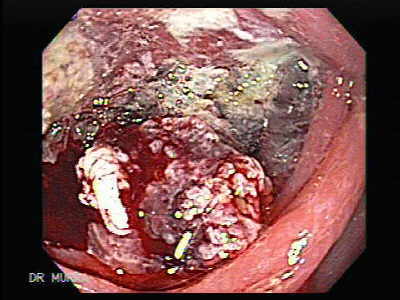
Video Endoscopic Sequence 1 of 5.
Adenocarcinoma of the Recto-Sigmoid junction with chicken skin mucosal changes
This a 50 year old male, who started with tenesmus, mucoid discharge with little bleeding, The colonoscopy found an ulcerated adenocarcinoma with chicken skin mucosal changes
Colonic chicken skin mucosa: an endoscopic and histological abnormality adjacent to colonic neoplasms.
is an endoscopic entity that occurs as a result of fat accumulation in macrophages in the lamina propria of the mucosa adjacent to colonic neoplasms. Small intestine-like microvilli were present in CSM and the pathophysiological implications remain to be elucidated.
CSMrelated adenoma was mainly found in the distal colon, and was associated with advanced pathology and multiple adenomas. CSM could be a potential predictive marker of the carcinogenetic progression of distally located colorectal adenomas.
Para mayores detalles descargar los videos presionando sobre las imágenes endoscópicas. Si los desea observar en pantalla completa, esperar a que se descargue completamente luego presionar Alt y Enter (pantalla completa).
Todas las imágenes endoscópicas de este Atlas contienen un video.
|
|
 |
Video Endoscopic Sequence 2 of 5.
Anterior to the tumor the mucosa is observed with chicken skin mucosal changes
|
|
 |
Video Endoscopic Sequence 3 of 5.
The tumor is somewhat invaginated but with some maneuver the colonoscope is advanced through the tumor some biopsies were taken.
|
|
 |
Video Endoscopic Sequence 4 of 5.
The distal part of the tumor, view from the colonoscope
|
|
 |
Video Endoscopic Sequence 5 of 5.
Posterior to the tumor, chicken skin mucosal changes is also observed. |
|
 |
Video Endoscopic Sequence 1 of 8.
Rectal Adenocarcinoma.
This 73 year-old man was referred to us by his surgeon due to palpable mass on digital rectal examination, colonoscopy confirm a large mass in the rectum.
This endoscopic image is seen at retroflexion
For more endoscopic details download the video clips by
clicking on the endoscopic images, wait to be downloaded
complete then press Alt and Enter; thus you can observe
the video in full screen.
All endoscopic images shown in this Atlas contain
video clips.
|
|
 |
Video Endoscopic Sequence 2 of 8.
Rectal Adenocarcinoma
Rectal tumors may be asymptomatic, but the possible symptoms of rectal tumors include the following
Palpable mass on digital rectal examination
Overt rectal bleeding
Microcytic anemia with fatigue, shortness of breath, and angina
Vague abdominal discomfort
Change in bowel habit
Large bowel obstruction
Pneumaturia
Feculent vaginal discharge
Perforation (rare)
Weight loss
Jaundice
Ascites
|
|
.
Perform complete colonoscopy looking for syncronic adenonocarcinoma or polyps.Colonoscopy, which has been found to be more accurate in detecting synchronous neoplasms, should be included in the evaluation of all patients with colorectal cancers.
Perform CT studies to stage the tumor before treatment and to choose the most appropriate treatment. Although magnetic resonance imaging (MRI) is slightly more accurate than CT in staging primary rectal tumors, CT is much more widely available. Most institutions and departments have more extensive experience using CT than MRI and continue to use CT for staging rectal tumors.
This may change in the future.") |
Video Endoscopic Sequence 3 of 8.
Endoscopic View of Rectal Adenocarcinoma
Evaluation begins with a history and physical examination, including a digital rectal examination.
Inspect the stool and test for occult blood.
Order blood tests (ie, complete blood count, liver function tests, and carcinoembryonic antigen levels).
Perform complete colonoscopy looking for syncronic adenonocarcinoma or polyps.Colonoscopy, which has been found to be more accurate in detecting synchronous neoplasms, should be included in the evaluation of all patients with colorectal cancers.
Perform CT studies to stage the tumor before treatment and to choose the most appropriate treatment. Although magnetic resonance imaging (MRI) is slightly more accurate than CT in staging primary rectal tumors, CT is much more widely available. Most institutions and departments have more extensive experience using CT than MRI and continue to use CT for staging rectal tumors.
This may change in the future.
|
|
 |
Video Endoscopic Sequence 4 of 8.
The neoplasia infiltrates immediately after the pectinea line
Many factors increase the risk for rectal cancer, including the following:
High-fat, low-fiber diet
Age greater than 50 years
Personal history of colorectal adenoma or carcinoma (3-fold greater risk).
First-degree relative with colorectal cancer (3-fold greater risk).
Familial polyposis coli, Gardner syndrome, and Turcot syndrome (in which all patients without a colectomy develop colorectal carcinoma).
Juvenile polyposis syndrome, Peutz-Jeghers syndrome, and Muir syndrome
(risk increased slightly).
Hereditary nonpolyposis colorectal cancer (as many as 50% of patients are affected).
Inflammatory bowel disease.
Ulcerative colitis (risk is 30% after 25 y)
Crohn disease (4- to 10-fold risk).
|
|
 |
Video Endoscopic Sequence 5 of 8.
The presentation depends on the site of the cancer:
Right colon cancers: weight loss, anemia, occult bleeding, mass in right iliac fossa, disease more likely to be advanced at presentation.
Left colon cancers: often colicky pain, rectal bleeding, bowel obstruction, tenesmus, mass in left iliac fossa, early change in bowel habit, less advanced disease at presentation.
The most common presenting symptoms and signs of cancer or large polyps are rectal bleeding, persisting change in bowel habit and anemia.
All patients with symptoms suspicious of colorectal cancer must have a thorough abdominal and rectal examination.
In some patients, symptoms do not become apparent until the cancer is far advanced. Approximately 55% of patients present with advanced colorectal cancer (spread to the lymph nodes, metastasised to other organs, or is so locally invasive that surgery to remove the primary tumour alone is unlikely to be sufficient for cure
Jaundice and hepatomegaly indicate advanced disease with extensive liver metastases. Peritoneal metastases with ascites are often also present. 20-25% of patients have clinically detectable liver metastases at the time of the initial diagnosis and a further 40-50% of patients develop liver metastases within three years of primary surgery.
Rarer clinical signs include: pneumaturia, gastro-colic fistula, ischiorectal or perineal abscesses, deep vein thrombosis.
|
|
 carcinoma, and have the best prognosis. The 5-year survival rate is approximately 50%. Screening for and removing adenomatous polyps may improve survival rates.") |
Video Endoscopic Sequence 6 of 8.
Endoscopic View of Rectal Cancer
Almost all rectal cancers are primary adenocarcinomas. Adenocarcinoma of the rectum is a major cause of mortality and morbidity in North America and Western Europe. Rectal cancers are, after colon cancers, the second most common gastrointestinal (GI) carcinoma, and have the best prognosis. The 5-year survival rate is approximately 50%. Screening for and removing adenomatous polyps may improve survival rates.
|
|
 |
Video Endoscopic Sequence 7 of 8.
Endoscopy of Rectal Cancer
Adenocarcinoma of the rectum arises as an intramucosal epithelial lesion, usually in an adenomatous polyp or gland. As cancers grow, they invade the muscularis mucosa, lymphatic structures, and vascular structures and involve regional lymph nodes, adjacent structures, and distant sites, especially the liver.
|
|
 |
Video Endoscopic Sequence 8 of 8.
Enhanced magnification colonoscopy.
|
|
 |
Video Endoscopic Sequence 1 of 12.
Colon Adenocarcinoma, Villous Adenocarcinoma.
Adenocarcinoma of the splenic flexure with villous component.
A 58 year-old male with weigh loss of 20 ponds and palpable mass in the upper left abdomen.
|
|
 microscope.") |
Video Endoscopic Sequence 2 of 12.
Endoscopic View of Colon Cancer
Endoscopic image with optical magnification.
Numerous finger like indentations forming a polypoid mass.
Magnification endoscopy, with or without dye spraying, has been developed for this purpose, allowing fine topographical details to be seen. The structures visible by magnification endoscopy correspond to those seen under a dissecting (stereoscopic) microscope.
|
|
 |
Video Endoscopic Sequence 3 of 12.
Chromoendoscopy using methylene blue.
Chromoendoscopy involves the topical application of stains or dyes to improve mucosal visualization during endoscopy.
|
|
 |
Video Endoscopic Sequence 4 of 12.
Another image and video clip of chromoendoscopy, using methylene blue.
|
|
 |
Video Endoscopic Sequence 5 of 12.
Microscopic specimen of the adenocarcinoma with villous componente.
Download the video clip by clicking on the image.
|
|
 |
Video Endoscopic Sequence 6 of 12.
Cancer of the Colon, Macroscopic specimen of the tumor.
|
|
 |
Video Endoscopic Sequence 7 of 12.
Cancer of the Colon, Macroscopic specimen of the tumor.
To enlarge the images in a new windows, click on them.
|
|
 |
Video Endoscopic Sequence 8 of 12.
Cancer of the Colon, Macroscopic specimen of the tumor.
|
|
 |
Video Endoscopic Sequence 9 of 12.
Cancer of the Colon. Macroscopic specimen
|
|
 |
Video Endoscopic Sequence 10 of 12.
Cancer of the Colon, Macroscopic specimen
|
|
 |
Video Endoscopic Sequence 11 of 12.
Cancer of the Colon, Macroscopic specimen
|
|
 |
Video Endoscopic Sequence 12 of 12.
Cancer of the Colon, Macroscopic specimen
|
|
 |
Rectal adenocarcinoma with acanthosis nigrans association.
A 73 year-old female, who was referred to us because of rectal blood discharge.
A constricting, ulcerated, annular rectal carcinoma was found.
The patient had severe the clinical picture of a severe acanthosis nigrans. In order to appreciate the pictures of this dermatologica associated cancer press here.
|
|
 |
Video Endoscopic Sequence 1 of 3.
Rectal cancer that emerges in the pectin line.
|
|
 |
Video Endoscopic Sequence 2 of 3.
Rectal Adenocarcinoma
The tumor is observed in retroflexed view.
|
|
 |
Video Endoscopic Sequence 3 of 3.
Same case as the one shown above.
|
|
 |
Video Endoscopic Sequence 1 of 5.
Rectal Adenocarcinoma that infiltrates the second and the third valve.
|
|
 |
Video Endoscopic Sequence 2 of 5.
The conoscope is advanced after the tumor finding an adenomatous polyp confirming adenoma-carcinoma theory.
In Colorectal Canceres At the time of surgical resection, it is important to ascertain preoperatively whether or not a second lesion exists. If synchronous polyps are present in patients with synchronous colorectal carcinomas, they should be ablated to reduce the risk of metachronous colorectal carcinoma.
|
|
 |
Sequence 3 of 5.
Rectal Cancer
Macroscopic specimen of the tumor.
|
|
 |
Sequence 4 of 5.
Rectal Cancer
Microscopic specimen of the adenocarcinoma.
|
|
 |
Sequence 5 of 5.
Rectal Cancer
Another view of the macroscopic specimen.
|
|
 |
Rectal Carcinoma at the Second Valve.
The video clip displays internal hemorrhoids.
It is a common situation that the medical history reveals when the patient had been under prior treatment for hemorrhoids, over a long period of time, without having a digital examination.
|
|
 |
Endoscopic Image of Adenocarcinoma of the Rectum
Circumferential neoplasia with an ulcerated center and everted edge.
|
|
 |
Rectum Adenocarcinoma.
This sessile lesion in the rectum presented with frank bleeding. The lesion was ulcerated in various places and bled heavily when touched.
|
|
 |
Video Endoscopic Sequence 1 of 3.
Endoscopic Image of Adenocarcinoma of the rectum.
A 66 year-old female with rectal adenocarcinoma that infiltrated from the first to the third rectal valve.
|
|
 |
Video Endoscopic Sequence 2 of 3.
Retroflexed maneuver was performed to evaluate the extension of the carcinoma.
|
|
 |
Video Endoscopic Sequence 3 of 3.
Endoscopic Image of Adenocarcinoma of the rectum.
Same case of above, the rectal tumor is observed in retroflexed view.
|
|
|
|
|
|
|





