 |
|
 |
Atrophic Gastritis
Atrophic gastritis is a histopathological entity characterized bychronic inflammation of the gastric mucosa with loss of gastricglandular cells and replacement by intestinal-type epithelium,pyloric-type glands, and fibrous tissue. Atrophy of the gastricmucosa is the endpoint of chronic processes, such as chronicgastritis associated with Helicobacter pylori infection, otherunidentified environmental factors, and autoimmunity directedagainst gastric glandular cells.
Atrophic gastritis represents the end stage of chronic gastritis,both infectious and autoimmune. In both cases, the clinica manifestations of atrophic gastritis are those of chronic gastritis,but pernicious anemia is observed specifically in patients withautoimmune gastritis and not in those with H pylori– associatedatrophic gastritis.
Acute H pylori infection usually is not detected clinically, but experimental infection results in a clinical syndrome characterized by epigastric pain, fullness, nausea, vomiting, flatulence, malaise, and, sometimes, fever. The symptoms resolve in approximately a week, regardless of whether H pylori organisms are eliminated.
Persistence of the organism causes H pylori chronic gastritis, which usually is asymptomatic or may manifest as gastric pain and, rarely, nausea, vomiting, anorexia, or significant weight loss. Symptoms associated with complications of chronic H pylori– associated atrophic gastritis may develop, including gastric ulcers and gastric adenocarcinoma.
For more endoscopic details download the video clips by clicking on the endoscopic images, wait to be downloaded complete then press Alt and Enter; thus you can observe the video in full screen.
All endoscopic images shown in this Atlas contain
video clips.
|
|
 |
Video Endoscopic Sequence 1 of 8.
Endoscopy of a Chronic Gastritis.
This 60 year-old male, pathologist, is under screening for
abdominal pain and jaundice. An upper endoscopy was
performed displaying this image and video clip.
Chronic gastritis with a depressed lesion was found that
had to rule out malignancy.
The Cat Scan displayed a Carcinoma of the head of the
pancreas.

|
|
 |
Video Endoscopic Sequence 2 of 8.
Image and video clip of Chronic Gastritis
A depressed lesion is seen, multiple biopsies were taken
to rule out a gastric adenocarcinoma.
|
|
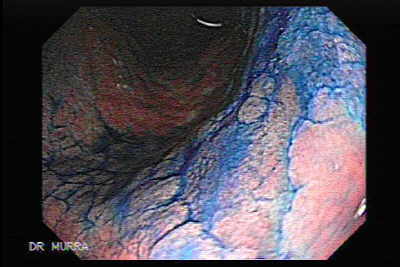 |
Video Endoscopic Sequence 3 of 8.
Image and video clip of Chronic Gastritis.
Chromoendoscopy using methylene blue.
|
|
 |
Video Endoscopic Sequence 4 of 8.
Image and video clip of Chronic Gastritis.
H pylori–associated chronic gastritis.
H pylori are gram-negative rods that have the ability to colonizeand infect the stomach. The bacteria survive within the mucouslayer that covers the gastric surface epithelium and the upperportions of the gastric foveolae. The infection usually is acquiredduring childhood. Once the organism has been acquired, haspassed through the mucous layer, and has become established atthe luminal surface of the stomach, an intense inflammatoryresponse of the underlying tissue develops.
|
|
 |
Video Endoscopic Sequence 5 of 8.
Image and video clip of Chronic Gastritis.
The presence of H pylori always is associated with tissue damageand the histological finding of both an active and chronic gastritis.The host response to H pylori and bacterial products iscomposed of T- and B-cell lymphocytes, denoting chronicgastritis, followed by infiltration of the lamina propria and gastricepithelium by polymorphonuclear leukocytes that eventuallyphagocytize the bacteria. The presence of polymorphonuclearleukocytes in the gastric mucosa is diagnostic of active gastritis.
|
|
 |
Video Endoscopic Sequence 6 of 8.
Image and video clip of Chronic Gastritis.
H pylori–associated chronic gastritis progresses with thefollowing 2 main topographic patterns that have different clinicalconsequences:
Antral predominant gastritis is characterized by inflammation and is mostly limited to the antrum. Individuals with peptic ulcers usually demonstrate this pattern of gastritis.
Multifocal atrophic gastritis is characterized by involvement of the corpus and gastric antrum with progressive development of gastric atrophy (loss of the gastric glands) and partial replacement of gastric glands by an intestinal-type epithelium (intestinal metaplasia). Individuals who develop gastric carcinoma and gastric ulcers usually demonstrate this pattern of gastritis.
Most of the people who are infected with H pylori do notdevelop significant clinical complications, and they remain carrierswith asymptomatic chronic gastritis. Some individuals who carryadditional risk factors may develop peptic ulcer, gastricmucosa–associated lymphoid tissue (MALT) lymphomas, orgastric adenocarcinomas.
|
|
 |
Video Endoscopic Sequence 7 of 8.
Image and video clip of Chronic Gastritis.
Some biopsies were taken to rule out adenocarcinoma.
|
|
 |
Video Endoscopic Sequence 8 of 8.
An enlarged bulging papilla was found, an ERCP was
performed.
The Cat Scan displayed a Carcinoma of the head of the
pancreas.
|
|
 and thehistopathological pattern, which may suggest the etiologicagent and clinical course (eg, H pyloriassociatedmultifocal atrophic gastritis). Other classifications arebased on the endoscopic appearance of the gastricmucosa (eg, varioliform gastritis). Although minimalinflammation is observed in some gastropathies, such asthose associated with NSAID intake, these entities arediscussed in this article because they are frequentlyincluded in the differential diagnosis of chronic gastritis.") |
Chronic Gastritis.
Image of chronic gastritis as observed the discoloration of
the mucosa.
Chronic gastritis, by definition, is a histopathologicalentity characterized by chronic inflammation of thestomach mucosa. Gastritis can be classified based onthe underlying etiologic agent (eg, Helicobacter pylori,bile reflux, nonsteroidal anti-inflammatory drugs[NSAIDs], autoimmunity, allergic response) and thehistopathological pattern, which may suggest the etiologicagent and clinical course (eg, H pylori–associatedmultifocal atrophic gastritis). Other classifications arebased on the endoscopic appearance of the gastricmucosa (eg, varioliform gastritis). Although minimalinflammation is observed in some gastropathies, such asthose associated with NSAID intake, these entities arediscussed in this article because they are frequentlyincluded in the differential diagnosis of chronic gastritis.
|
|
 |
Video Endoscopic Sequence 1 of 2.
Gastric Erosion.
Seen with magnification and high-resolution
chromoendoscopy.
H.Pylori infection was found in the biopsies.
Helicobacter pylori is the major cause of chronic gastritis
worldwide. With an estimated rate of infection of over one
half of the world's population, it is responsible for
extensive morbidity and mortality. Infection with this
organism does not appear to spontaneously resolve.
Instead it reaches a chronic stage from which a number of
outcomes are possible.
|
|
, with the antrum being speared. In contrast,
chronic atrophic gastritis consequent to H. pylori infection
is a multifocal pangastritis, involving independent foci in
the corpus and antrum of the stomach.") |
Video Endoscopic Sequence 2 of 2.
Cronic Gastritis
Furrow of erosioned mucosal changes.
Gastric carcinoma of the intestinal type originates in dysplastic epithelium, which in turn develops in the milieu of atrophic gastritis and intestinal metaplasia. Cancers also may develop less often from gastric adenomatous polyps, which represent dysplastic epithelium arising in a raised lesion. The main causes of chronic atrophic gastritis and gastric atrophy are autoimmune due to pernicious anemia or chronic Helicobacter pylori infection. In the former condition, there is severe atrophy of the corpus (oxyntic mucosa), with the antrum being speared. In contrast, chronic atrophic gastritis consequent to H. pylori infection is a multifocal pangastritis, involving independent foci in the corpus and antrum of the stomach.
|
|
 nodules, some with central
depression or erosions, are observed. The cause of this
uncommon entity is unknown and reflects a chronic erosive
inflammatory process.") |
Chronic Variliform ( chronic erosive ) Gastritis.
Multiples small (5-10 mm) nodules, some with central
depression or erosions, are observed. The cause of this
uncommon entity is unknown and reflects a chronic erosive
inflammatory process.
|
|
 is an
uncommon and rarely reported disorder affecting various
parts of the gastrointestinal (GI) tract. The disease is
defined as a disorder characterized by eosinophilic
infiltration of one or more areas of GI tract in the absence
of any known cause of eosinophilia and exclusion of
eosinophilic infiltrations in organs other than gut.
Depending upon the area involved, the disease can present
as eosinophilic esophagitis, oeosinophilic gastritis (EG),
eosinophilic gastroenteritis (EGE) or eosinophilic colitis.") |
Video Endoscopic Sequence 1 of 7.
Eosinophilic Gastritis
Endoscopic features of Eosinophilic Gastritismay include
prominent mucosal folds, hyperemia, ulcerations or
nodularity.
Eosinophilic Gastrointestinal disorder (EGID) is an
uncommon and rarely reported disorder affecting various
parts of the gastrointestinal (GI) tract. The disease is
defined as a disorder characterized by eosinophilic
infiltration of one or more areas of GI tract in the absence
of any known cause of eosinophilia and exclusion of
eosinophilic infiltrations in organs other than gut.
Depending upon the area involved, the disease can present
as eosinophilic esophagitis, oeosinophilic gastritis (EG),
eosinophilic gastroenteritis (EGE) or eosinophilic colitis.
|
|
 |
Video Endoscopic Sequence 2 of 7.
Eosinophilic Gastritis
The exact pathophysiology of the disease is unknown, but
is associated with selective infiltration of eosinophils in
parts of GI tract.
Eosinophilic gastritis is rare disorder and can present with
a variety of symptoms. The physicians should have a high
index of suspicion in patients presenting with
uncharacteristic symptoms or unresponsive to
conventional therapy. Histological confirmation is essential
for diagnosis. The disease needs to be differentiated from
generalized eosinophilic disorder presenting with organ
involvement other than GI tract.
Currently the steroids appear to be the main stay of
treatment, but most patient relapse after withdrawal of
treatment.
|
|
 |
Video Endoscopic Sequence 3 of 7.
Endoscopy and histopthological examination of the
biopsies are an essential part of the diagnostic work-up.
|
|
 |
Video Endoscopic Sequence 4 of 7.
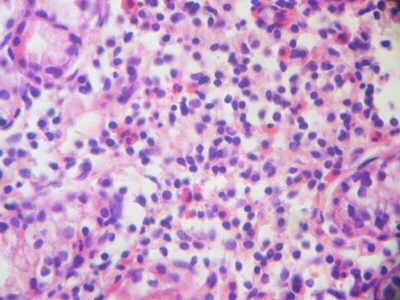
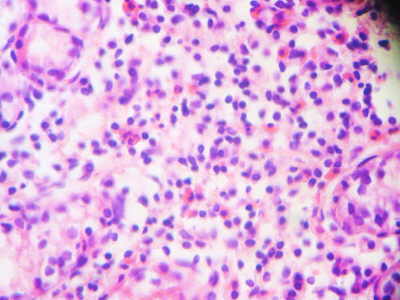
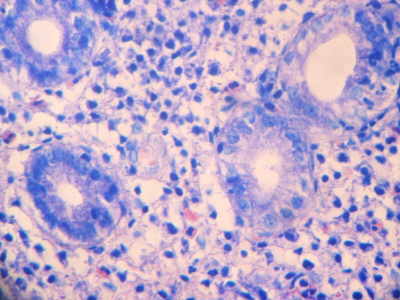
Histology is the ‘gold standard’ for diagnosis of EGE.
Common histological features includes increase number of
eosinophils (>50/HPF) in lamina propia. Large number of
eosinophils may also be present in the muscularis and
serosal layer which may produce crypt hyperplasia,
epithelial cell necrosis and villous atrophy.
|
|
 |
Video Endoscopic Sequence 5 of 7.
|
|
 |
Video Endoscopic Sequence 6 of 7. |
|
 |
|

|
Atrophic Gastritis
Atrophic gastritis is a histopathologic entity characterized by chronic inflammation of the gastric mucosa with loss of gastric glandular cells and replacement by intestinal-type epithelium, pyloric-type glands, and fibrous tissue. Atrophy of the gastric mucosa is the endpoint of chronic processes, such as chronic gastritis associated with Helicobacter pylori infection, other unidentified environmental factors, and autoimmunity directed against gastric glandular cells.
The 2 main causes of atrophic gastritis result in distinct topographic types of gastritis, which can be distinguished histologically. H pylori- associated atrophic gastritis is usually a multifocal process that involves both the antrum and oxyntic mucosa of the gastric corpus and fundus, whereas autoimmune gastritis essentially is restricted to the gastric corpus and fundus. Individuals with autoimmune gastritis may develop pernicious anemia because of extensive loss of parietal cell mass and anti-intrinsic factor antibodies.
H pylori- associated atrophic gastritis is frequently asymptomatic, but individuals with this disease are at increased risk of developing gastric carcinoma, which may decrease following H pylori eradication. Patients with chronic atrophic gastritis develop low gastric acid output and hypergastrinemia, which may lead to enterochromaffin-like (ECL) cell hyperplasia and carcinoid tumors.
H pylori are gram-negative bacteria that colonize and infect the stomach. The bacteria lodge within the mucous layer of the stomach along the gastric surface epithelium and the upper portions of the gastric foveolae and rarely are present in the deeper glands.
Atrophic gastritis. Schematic representation of Helicobacter pylori–associated patterns of gastritis. Involvement of the corpus, fundus, and gastric antrum, with progressive development of gastric atrophy as a result of loss of gastric glands and partial replacement of gastric glands by intestinal-type epithelium, or intestinal metaplasia (represented by the blue areas in the diagram) characterize multifocal atrophic gastritis. Individuals who develop gastric carcinoma and gastric ulcers usually present with this pattern of gastritis. Inflammation mostly limited to the antrum characterizes antral-predominant gastritis. Individuals with peptic ulcers usually develop this pattern of gastritis, and it is the most frequent pattern in Western countries.
|
|
|
|
|
|
|