 |
|
 |
Video Endoscopic Sequence 1 of 10.
Flexible Endoscopic Suturing.
A 24 year-old female, suffering of GERD due to inferior gastroesophageal sphincter incompetence.
The patient has these symptoms since 7 years, even using PPI.
To overcome the GERD an Endoscopic Anti-Reflux Procedure was performed see below the complete sequence of images and videos clips
For further endoscopic information, download the video clip by clicking on the endoscopic image. Wait to be downloaded complete then Press Alt and Enter for full screen ( Windows Media), Real Player: Ctrl and 3.
All endoscopic images shown in this Atlas contain video clips. We recommend seeing the video clips in full screen mode.
|
|
.") |
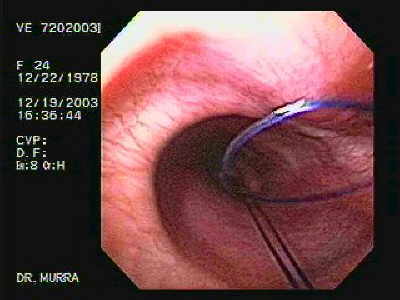
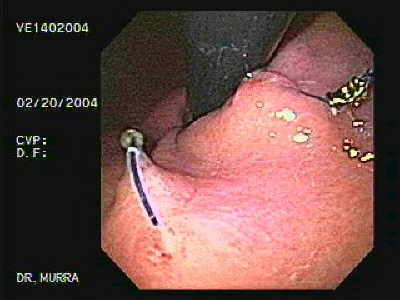
Video Endoscopic Sequence 2 of 10.
Endoscopic Anti-Reflux Procedure.
The image and the video a flexible device with treads is shown, the tip of flexible endoscopic (flexible Sew-Right Device).
|
|
 |
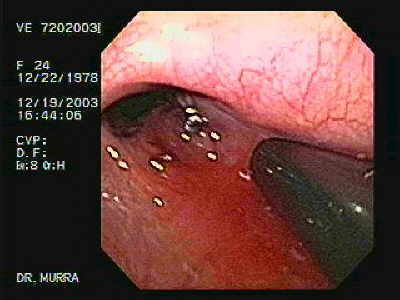
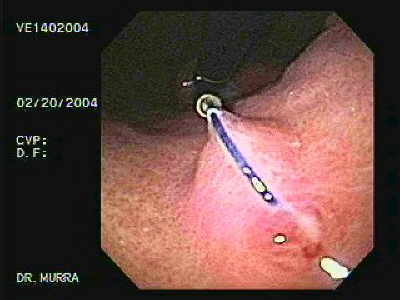
Video Endoscopic Sequence 3 of 10.
Flexible Endoscopic Suturing.
Clamp with threads is suctioning the gastroesophageal junction.
|
|
 with gently movements is withdrawing.") |
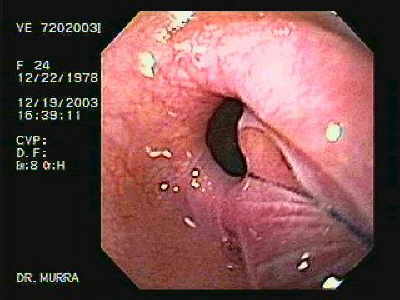
Video Endoscopic Sequence 4 of 10.
Endoscopic Anti-Reflux Procedure.
The video clip displays the flexible Sew-Right Device has been released the tissues (the suction is turned off) with gently movements is withdrawing.
|
|
 |
Video Endoscopic Sequence 5 of 10.
Endoscopic Anti-Reflux Procedure.
4 treads are observed after traction is performed, they will become in 2, after that a titanium clip will be placed to perform the knot.
|
|
 |
Video Endoscopic Sequence 6 of 10.
The 4 threads has been converted in 2.
|
|
 |
Video Endoscopic Sequence 7 of 10.
The image and the video clip display the traction exerted
by the treads that tied the tissues.
|
|
 |
Video Endoscopic Sequence 8 of 10.
The flexible Ti-Knot Device has been placed the titanium
clip performing the knot.
|
|
 |
Video Endoscopic Sequence 9 of 10.
The gastroplication has been completed. Plication techniques create a mechanical barrier to reflux through apposition of 2 mucosal surfaces at the gastroesophageal junction or in the cardia.
The mechanisms as to how endoscopic suturing might improve competence of the gastroesophageal junction, however, remain unclear.
The manometric studies that are available are conflicting. Some have reported an increase in basal lower esophageal sphincter (LES) pressure andlength.
A multicenter study, however, found no impact on sample measures of LES function in reflux disease patients despite evidence of symptom benefit.
|
|
 |
Video Endoscopic Sequence 10 of 10.
Final statust of the endoscopic gastroplicature.
Patient relief the symptoms.
Plication of the gastroesophageal junction by endoscopic
suturing has been reported to improve symptoms and
reduce acid exposure in patients with gastroesophageal
reflux disease (GERD).
|
|
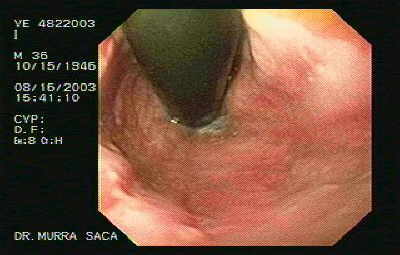 |
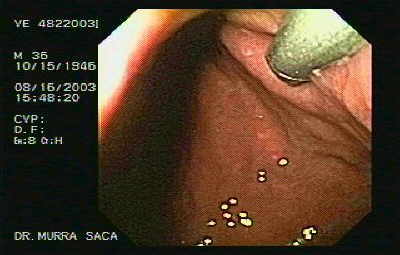
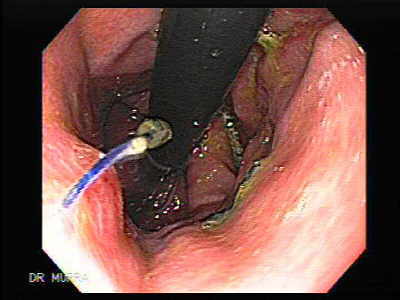
Video Endoscopic Sequence 1 of 11.
FLEXIBLE ENDOSCOPIC SUTURING DEVICE.
Endoscopic Suturing due to chronic gastroesophageal
reflux.
The image and the video display a retroflexed hiatal hernia.
A 35 year-old male, who has been suffering of
suffering refracting Gastro Esophageal Reflux Disease
(GERD) for the last 4 years.
|
|
 |
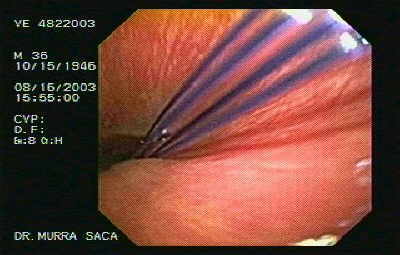
Video Endoscopic Sequence 2 of 11.
Suturing System and standard video endoscopy, sutures
are placed in the upper part of the stomach at or just below
the LES.
Two stitches can be placed and tied together to create a pleat near the LES and treat symptomatic reflux. The image and the video clip display a flexible suturing device which has been passed through the external accessory channel, with a friction-fit adapter and tube guide, provides a pathway for the flexible endoscopic suturing device
|
|
 |
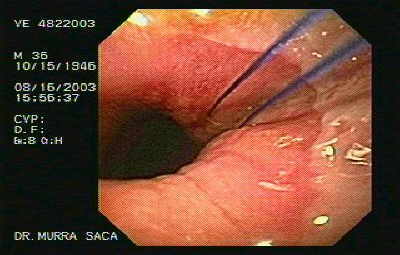
Video Endoscopic Sequence 3 of 11.
The ESD Flexible Endoscopic Suturing device. It uses the same principal of tightening the junction between the esophagus and the stomach by the placement of sutures.
This device has been approved by the FDA and is being studied for the treatment of GERD.
The image and the video display the step of sucking enough tissue (mucosa, sub mucosa and muscularis). The needle is then fired into the sucked tissue.
We applied the first suture with the first needle and at the same time we removed the valve of suction and in this way it free the tissue from the pincer and we prepared the field for the second suture which is one centimeter away from the first one.
|
|
 |
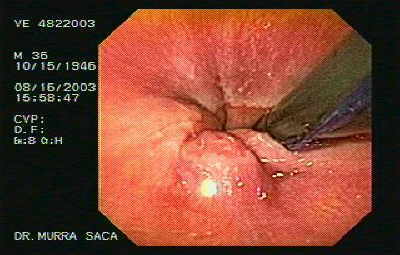
Video Endoscopic Sequence 4 of 11.
The image and the video clip display to loosen the tissues, certain maneuvers are observed, we prepared the second suture one centimeter away from the first one.
In the image observed the process after the tissue which deliver one suture, with this device.
We observed the threads through the cardias and then, we applied the second suture to one centimeter away from the first one. As we look the 4 threads that convert to two with applied traction that is direct out and both tissues gathered.
|
|
 |
Video Endoscopic Sequence 5 of 11.
We prepared the second suture one centimeter away from the first one. In the image observed the process after the tissue which we deliver one suture, with this device.
We observed the threads through the cardias and then, we applied the second suture to one centimeter away from the first one.
|
|
 |
Video Endoscopic Sequence 6 of 11.
We look the 4 threads that convert to two with applied
traction that is direct out and both tissues gathered
together. |
|
 |
Video Endoscopic Sequence 7 of 11.
The image and the video are displaying both threads that were observed as four, This happened because they were tractioned outwards.
In the image show two threads that previously were four, but after we applied outside traction and the cardia's tissue is suture and close to each other the next step is to tie between the sutures and we use other special forceps which we thread the needle in this pincer with a titanium's clip.
And we gaze the other flexible forceps which has the threads attach with a titanium's clip. |
|
 |
Video Endoscopic Sequence 8 of 11.
The next step is to perform the knot. The titanium knot mechanically fastens suture together and cuts away excess suture. And those threads position close to the mouth and out from the patient are introducing to other special pincer which is flexible to attach a titanium's clip.
|
|
 |
Video Endoscopic Sequence 9 of 11.
For more endoscopic details download the video clip by
clicking on the endoscopic images.
|
|
 |
Video Endoscopic Sequence 10 of 11.
In this step this clamp is withdrawn, the hole of the clamp is observed where the titanium knot is applied and the threads are cut, also this clamp is equipped to cut threads.
|
|
 |
Video Endoscopic Sequence 11 of 11.
The knot is observed, the threads and the titanium clip The first stich is finish of this form increase the pressure of the inferior gastroesophageal sphincter, this procedure is simple, two to four stitches are required according to the size of the hiatal hernia.
This endoscopic procedure is practical and safe. However, since this procedure is quite new, we can not determine at the moment its lasting effects.
Because of the patient’s benefits, due to the disappearance of gastroesophageal refluxe.
|
|
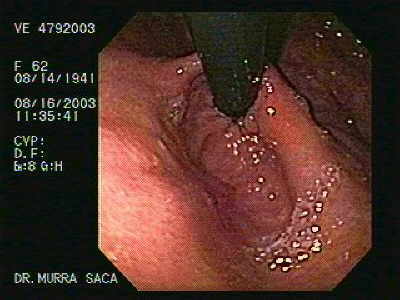 |
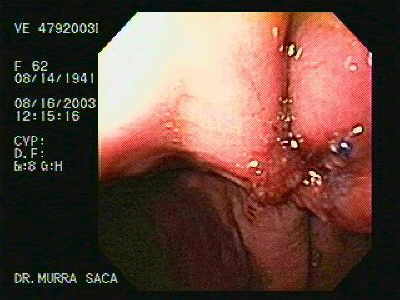
Video Endoscopic Sequence 1 of 14.
Intraluminal Endoscopic Suturing.
A 62 year-old female who has been presenting gastroesophageal reflux for 8 years.
A hernia of the hiatus with an extended defect is observed which affects the closing mechanism and contributes to the gastroesophageal reflux.
Two endoscopic gastroplicaturas were placed.
|
|
|
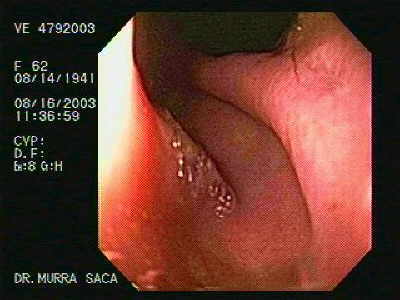 |
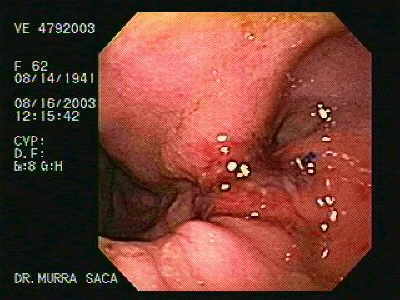
Video Endoscopic Sequence 2 of 14.
In the video clip an hiatus hernia with a defect is observed.
Endoscopic suturing causes modest but significant improvement in LES function.
First, there is a significant reduction in the triggering of transient LES relaxations (tLESRs) and second, there is a small but significant increase in basal LES pressure. Overall, tLESRs were reduced by 37% at 6 months, but the overall number of reflux episodes was unchanged and there was only a modest decrease in upright GER (14.4% to 9.2%, median values at baseline and 6 months, p< 0.05) and no change in supine reflux.
Nevertheless, 7 of 15 (45%) patients were free of symptoms and off medication at 1 yr and 4 of 15 (26%) patients had normal pH values. The speculated mechanism of these changes was twofold. First, the plication and possibly associated scarring just below the squamocolumnar junction may reduce the distensibilty of the cardia region of the stomach, the recognized trigger zone for tLESRs. Secondly, scarring may also affect neural pathways, thereby reducing the rate of tLESRs.
|
|
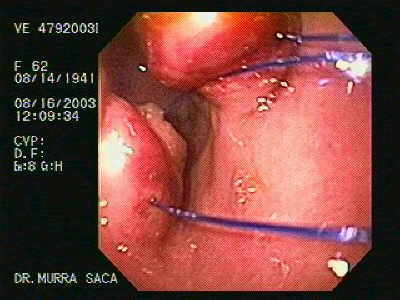 |
Video Endoscopic Sequence 3 of 14.
The threads are observed which approaching the tissues.
|
|
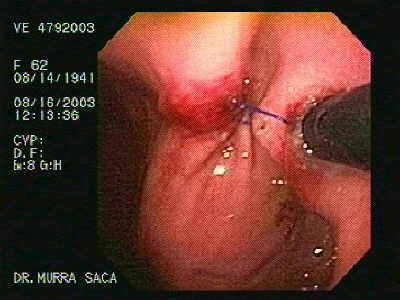 |
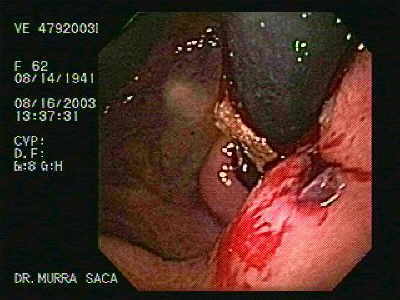
Video Endoscopic Sequence 4 of 14.
In the image and the video clip you can see the placement
of the titanium clip through the clamp performing the first
gastroplicature in this patient.
|
|
 |
Video Endoscopic Sequence 5 of 14.
This image and the video clip display the first intraluminal
gastroplicature.
|
|
 |
Video Endoscopic Sequence 6 of 14.
Another appreciation of the endoluminal gastroplicature.
|
|
 |
Video Endoscopic Sequence 7 of 14.
Retroflexed image of the gastric fundus the final status of
this procedure. |
|
 |
Video Endoscopic Sequence 8 of 14.
Transoral Endoluminal Gastroplications
A follow up after six months. We practiced two endoscopicEndoluminal Gastroplications.
She has been our first patient with this new endoscopic suturing method. After the endoscopic gastroplicatures, patient has not reported any GERD symptom and not get any anti reflux drug.
|
|
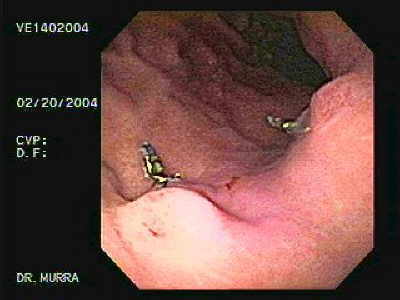 |
Video Endoscopic Sequence 9 of 14.
The image and the video clip display two nodules as
results of previously endoluminal gastroplicature six
months ago. Two clips of titanium are observed.
|
|
 |
Video Endoscopic Sequence 10 of 14.
Retroflexed image, where two nodules can be seen. These nodules were formed with the junction of the tissues, Besides, an inflammatory reaction is observed, due to foreign body reaction to the nylon thread, which apparently is useful for increasing the resistance of the sphincter therefore avoiding the reflux, which is the purpose of the procedure.
We have one case of silk thread remains, after a gastric surgery performed 20 years ago. The silk thread caused the mucosa inflammatory reaction as a consequence of foreign body reaction see post surgical status.
|
|
 |
Video Endoscopic Sequence 11 of 14.
In this retroflexed image are observed two nodules of the
endoscopic gastroplicature. |
|
 |
Video Endoscopic Sequence 12 of 14.
In this image we can appreciate the nodule with some foreign body reaction to the nylon thread.
This seems to facilitate the development of the fibrosis and increase the resistance of the sphincter.
Until now we have had a very good experience withthe intraluminal endoscopic suture, since the patients have had a very good results; the acidity has disappeared and we hoped that this effect will remain for a long time.
However, only the time will tell the final word, since so far this method has been proved effective, in spite of being new.
|
|
 |
Video Endoscopic Sequence 13 of 14.
A follow up one year after.
|
|
 |
Video Endoscopic Sequence 14 of 14.
A follow up one year after.
Retroflexed maneuver.
|
|
 |
Image of the suture after five years
|
|
|
|
|
|
|