 |
|
 |
Intragastric Ant
This naughty ant is moving inside the stomach of a patient, a surprise that an endoscopist can have.
Here displays, how powerful the stomach acid is shown in defend against certain germs.
When we were practicing endoscopy and wash secretions on a cholesteatoma note this ant which moves within the gastric camera
and within seconds dies due to the effect of the powerful gastric acid.
Ant passes through the working channel of the endoscope is in the water tank which is used to wash the secretions and also is used for wash through the working channel.
For more endoscopic details download the video clips by
clicking on the endoscopic images, wait to be downloaded
complete then press Alt and Enter; thus you can observe
the video in full screen.
All endoscopic images shown in this Atlas contain
video clips.
|
|
 |
Video Endoscopic Sequence 1 of 10.
Extrinsic compression due to malign ascites
This 34 year-old male that, two years previously was
diagnosed as having colon cancer, now present a severe
abdominal bulking due to a malign ascites.
|
|
 |
Video Endoscopic Sequence 2 of 10.
At the gastric fundus is observed two extrinsic compression
|
|
 |
Video Endoscopic Sequence 3 of 10.
In order to relief the ascites a transgastric procedure was
performed, first a pre-cut needle was used through an
duodenoscope.
|
|
 |
Video Endoscopic Sequence 4 of 10.
After the gastric walls was opened a hydrostatic balloon
was used to dilate the small hole.
|
|
 |
Video Endoscopic Sequence 5 of 10.
The gastric wall was open using a sphincterotome, te video
clip shows the ascites draining across the gastric wall, the
Intra-abdominal pressure was overcome.
|
|
 |
Video Endoscopic Sequence 6 of 10.
A pulsatile bleeding emerging from the gastric wall.
|
|
 |
Video Endoscopic Sequence 7 of 10.
To perform the hemostasis the argon plasma coagulator
was used combined with the absolute alcohol.
|
|
 |
Video Endoscopic Sequence 8 of 10.
Injection therapy with absolute alcohol.
|
|
 |
Video Endoscopic Sequence 9 of 10.
After the gastric wall is open, a transgastric endoscopic
access of the peritoneal cavity is seen in the video clip.
|
|
 |
Video Endoscopic Sequence 10 of 10.
A transgastric periteneoscopy, a part of the peritoneal
cavity is observed.
|
|
 |
Video Endoscopic Sequence 1 of 8.
Gastric Carcinoid Tumor.
Carcinoids are the most common neuroendocrine tumors.
The tumor is derived from primitive stem cells in the gut
wall but can be seen in the liver, pancreas, bronchus, and
ovaries. In children, most cases occur in the appendix, and
most are benign and asymptomatic.
|
|
 |
Video Endoscopic Sequence 2 of 8.
Gastric Carcinoid Tumor.
These tumors have a yellow, tan, or gray-brownappearance
that can be observed through the intact mucosa. The yellow
color is a result of cholesterol and lipid accumulation within
the tumor. Tumors can have a polypoid appearance and
occasionally can ulcerate.
Similar images of Duodenal Carcinoid Tumor are found in
duodenal miscellaneous chapter.
|
|
 |
Video Endoscopic Sequence 3 of 8.
Gastric Carcinoid Tumor.
|
|
 |
Video Endoscopic Sequence 4 of 8.
Gastric Carcinoid Tumor.
Indigo Carmin Stain.
|
|
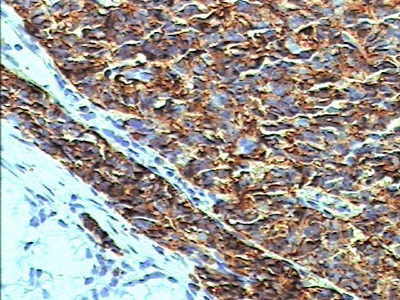 |
Video Endoscopic Sequence 5 of 8.
Cromogranina.
|
|
 |
Video Endoscopic Sequence 6 of 8.
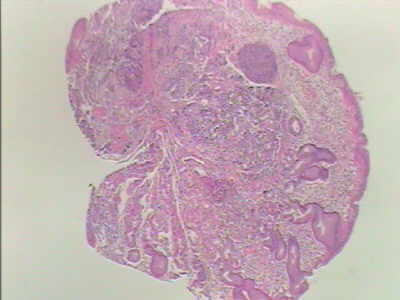
4x.
Gastric Carcinoid Tumor.
At low power there is an intramucosal neoplasia.
|
|
 |
Video Endoscopic Sequence 7 of 8.
10x.
Carcinoid Tumor.
At medium power the organoid neoplasia replace the
gastric glands. carcinoid tumor.
|
|
 |
Video Endoscopic Sequence 8 of 8.
40x.
The appendix is the most common site of gut carcinoid
tumor, followed by the small intestine, rectum, stomach and
ileum.
Carcinoid tumor are potentially malignant and the tendency
of malignant behavior correlate with the site of origin, the
depth of local penetration and the size of the tumor.
|
|
 |
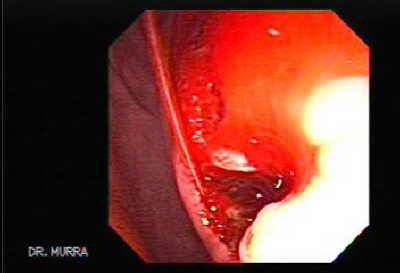
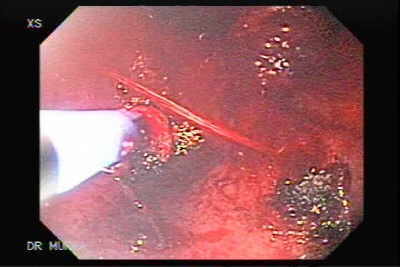
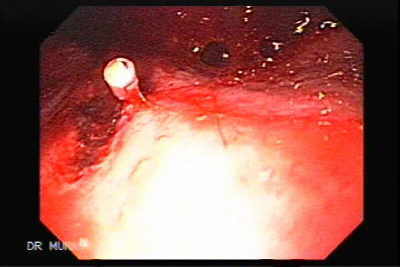
Video Endoscopic Sequence 1 of 7.
Severe Bleeding After Biopsies
A 91 year-old male 10 years before underwent a subtotal
gastrectomy due to gastric adenocarcinoma of the antrum
recently appeared a mass in the pancreato-biliary tree
causing jaundice, An endoscopy is performed to looking for
tumor regression, near the gastro-jejuno anastomosis had
an elevated area that it looks like a scar, multiple biopsies
were taken with jumbo forceps causing severe bleeding.
|
|
 |
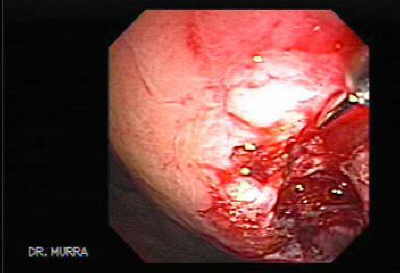
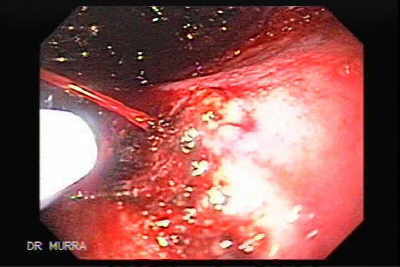
Video Endoscopic Sequence 2 of 7.
The bleeding was of severe intensity, at the beginning we used argon plasma coagulator.
|
|
 |
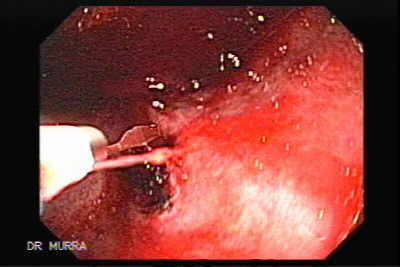
Video Endoscopic Sequence 3 of 7.
The argon plasma coagulator was not enough, as it was a
large caliber vessel, at this time we made the choice to use
between the dual-channel therapeutic endoscope with
argon plasma using therapeutic probe (larger caliber) or
infiltrate this vessel with absolute alcohol, deciding for the
latter.
|
|
 |
Video Endoscopic Sequence 4 of 7.
Injection of absolute alcohol was used in the area of the
vessel but also was no successful.
|
|
 |
Video Endoscopic Sequence 5 of 7.
After using the two therapies for hemostatic maneuver, a hemoclip was applied succeeding in stopping the bleeding
|
|
 |
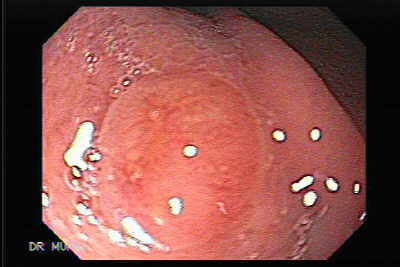
Video Endoscopic Sequence 6 of 7.
Final State of hemostatic therapy
|
|
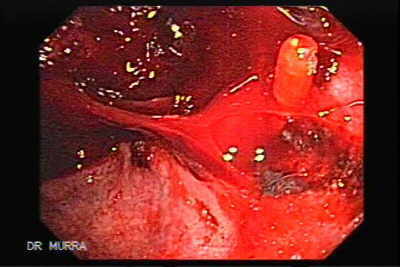 |
Video Endoscopic Sequence 7 of 7.
Another image and video clip of Final Status of hemostatic therapy.
Important Comments: In the professional practice in
almost all therapeutic procedures there are risks of
complications as in this case that there was a need of
taking biopsies taken as large forceps small malignant
lesions often are not demonstrated by the shortage of
tissues which is recommended to obtain macro-biopsies
but these can take the risk of bleeding in this case, but
success of this profession is to manage the
complications with certainty, having multiple resources
in hand as therapeutic and ablative therapies and
homeostatic, the endoscopist should have adequate training
and courage as well as the assistants.
|
|
 |
Foreign body.
Chewed gum in the stomach.
Patient swallowed the gum while in the waiting room.
|
|
 |
Phytobezoar.
Bezoars are concretions in the GI tract that increase in size by the accumulation of nonabsorbable food or fibers. They are uncommon, but when present, they are usually found in patients with altered GI motility or with a history of gastric surgery.
A phytobezoar is composed of indigested plant or vegetable fibres, plant skins and leaves. A phytobezoar may develop when foreign material accumulates in the stomach because of indigestibility, poor mastication or disturbances in the gastric emptying mechanism which can occur following surgical procedures such as vagotomy, pyloroplasty or antrectomy. A trichobezoar is secondary to hair ingestion, usually in mentally disturbed patients.
|
|
 |
Video Endoscopic Sequence 1 of 3.
Upside-Down Stomach
(Gastric Rotation)
The term "gastric volvulus" is reserved for cases in which
the abnormal rotation has led to strangulation and
obstruction Gastric volvulus is defined as an abnormal
rotation of the stomach of more than 180°, creating a
closed loop obstruction that can result in incarceration and
strangulation.
The stomach can rotate along an axis that is 90° to the
longitudinal axis. Such rotation is called a mesenteroaxial
rotation . This rotation may lead to an upside-down
stomach.
Mesenteroaxial rotation of an intrathoracic stomach is less
common than organoaxial rotation. Mesenteroaxial
rotation is more frequently seen in patients with
progression of a type 2 paraesophageal hiatal hernia.
|
|
 |
Video Endoscopic Sequence 2 of 3.
The most common cause of gastric volvulus in adults is
diaphragmatic defects. In cases of paraesophageal hernias,
the gastroesophageal junction remains in the abdomen
while the stomach ascends adjacent to the esophagus,
resulting in an upside-down stomach. Gastric volvulus is
the most common complication of paraesophageal hernias.
It has also been reported to complicate gastroesophageal
surgery, neuromuscular disorders, and intra-abdominal
tumors. Rarely, gastric volvulus may be a complication of
liver transplant and may be related to ligation of the
hepatogastric ligament during the hepatectomy.
|
|
 |
Video Endoscopic Sequence 3 of 3. |
|
 |
Video Endoscopic Sequence 1 of 7.
Non-specific finding in the gastric fundus in a lupus patient´s
This 54 year-old female with systemic lupus
erythaematosus presenting with abdominal pain, physical
Examination the abdomen soft, nontender, no masses,
hernias or organomegaly, two months previously had
discontinued her treatment with corticosteroids.
|
|
 |
Video Endoscopic Sequence 2 of 7.
Systemic lupus erythematosus (SLE) is a chronic
inflammatory disease of unknown cause that affects
multiple organ systems. Immunologic abnormalities,
especially the production of a number of antinuclear
antibodies, are another prominent feature of this disease.
The clinical course is marked by spontaneous remissions
and relapses. Its multisystemic manifestations and the
complications from the use of immunosuppressive agents
make the diagnosis and management of this entity
challenging.
|
|
 |
Video Endoscopic Sequence 3 of 7.
Gastric Erosion is observed the biopsies were negative to malignancy.
Gastrointestinal (GI) manifestations are common in
patients with systemic lupus erythematosus (SLE).
Virtually all patients with SLE require treatment with
NSAID therapy and/or corticosteroids
The ulcerogenic effects of NSAIDs and corticosteroids
used in combination are synergistic and put the patient at
a high risk of serious ulcer disease. In addition, high-dose
steroids may mask the early clinical signs of peptic ulcer
perforation.
|
|
 |
Video Endoscopic Sequence 4 of 7.
Systemic lupus erythematosus: Gastrointestinal Tract
Problems: Impairment of blood supply to various parts of
the gastrointestinal tract may result in abdominal pain,
damage to the liver or pancreas (pancreatitis), or a
blockage or tear (perforation) of the gastrointestinal tract.
|
|
 |
Secuencia Video Endoscópica 5 de 7.
The inflammatory infiltrate from patients with SLE was found to contain higher levels of young and mature fibroblasts than those from patients with gastroduodenitis, and was associated with the progression of SLE. During disease exacerbation, immune complex deposition was observed in the arteriolar walls
The inflammatory changes in the gastric and duodenal mucosa were ascertained to be associated with the progression of SLE. In exacerbation of SLE, the walls of vessels (arterioles) exhibited immune complexes classified mainly as IgG and, to a lesser degree, as IgM. In remission, the luminescence of the vessels decreased. The serum level of immunoglobins did not correlate with their regional production in the gastric and duodenal mucosa. |
|
 |
Video Endoscopic Sequence 6 of 7.
Systemic lupus erythematosus (SLE) on the
gastrointestinal (GI) tract from mouth to anus, attempting
to distinguish the features that are most likely to be due to
therapy. GI manifestations of SLE include mouth ulcers,
dysphagia, anorexia, nausea, vomiting, hemorrhage and
abdominal pain. GI vasculitis is usually accompanied by
evidence of active disease in other organs. Early
recognition of the significance of these symptoms offers
the best opportunity.
|
|
 |
Secuencia Video Endoscópica 7 de 7.
The inflammatory infiltrate from patients with SLE was found to contain higher levels of young and mature fibroblasts than those from patients with gastroduodenitis, and was associated with the progression of SLE. During disease exacerbation, immune complex deposition was observed in the arteriolar walls |
|
 |
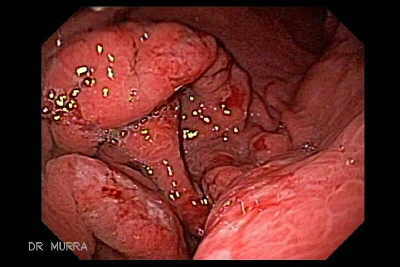
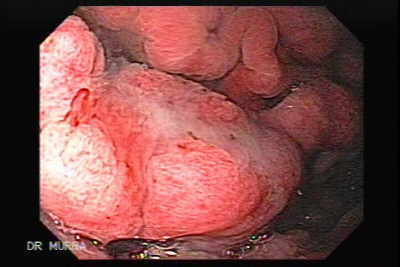
Video Endoscopic Sequence 1 of 24.
Menetrier's disease (Hypertrophic Gastropathy)
This 53 year-old male presented with abdominal pain, nausea weight loss of 20 libs
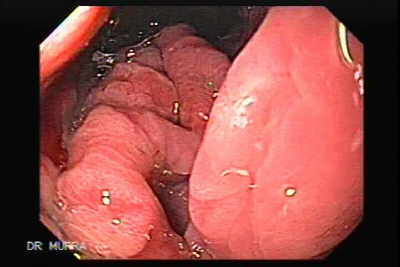
There are irregular thickened and large gastric folds of
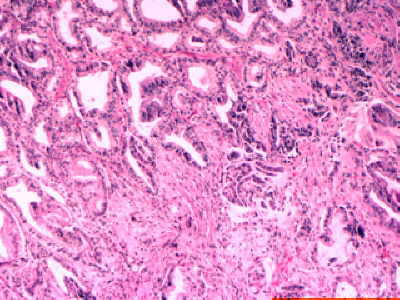
the fundus and proximal body two endoscopies showed
small foci of adenocarcinoma at first thought it was a
lymphoma or linitis plastica.
|
|
 |
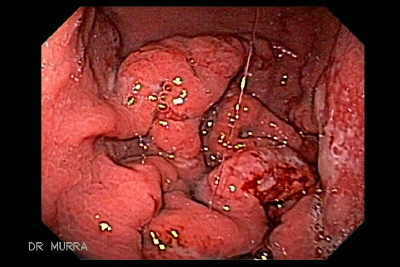
Video Endoscopic Sequence 2 of 24.
Menetrier disease is a rare disorder characterized by massive overgrowth of mucous cells (foveola) in the mucous membrane lining the stomach, resulting in large gastric folds. The main symptom associated with Menetrier disease is pain in the upper middle region of the stomach (epigastric pain). Premalignant disorder. The cause of Menetrier disease is unknown.
There is great variation in the thickness and configuration of normal gastric rugae. Endoscopists and radiologists therefore tend to overdiagnose Ménétrier's disease . In this rare disorder there is marked thickening , tortuosity and irregularity of the mucosal ridges, occasionally giving the mucosa an appearance suggestive of polyposis. Accurate diagnosis must be based on a combination of endoscopic and histopathological appearances.
|
|
 |
Video Endoscopic Sequence 3 of 24.
There is considerable confusion and contradiction in the
medical literature regarding disorders involving large
gastric folds. The name Menetrier disease is often
erroneously used to describe any condition with large
gastric folds or as a synonym for giant hypertrophic
gastritis (GHG). However, Menetrier disease is not a true
form of gastritis. A diagnosis of Menetrier disease should
be reserved for individuals with large gastric folds due to
overgrowth of mucous cells. There is minimal or no
stomach inflammation in Menetrier disease. Because
inflammation is minimal or not present, Menetrier disease
is classified as a form of hyperplastic gastropathy and not
as a form of gastritis. Some researchers believe that
Menetrier disease and GHG may be variants of the same
disorder or different parts of one disease spectrum.
|
|
 |
Video Endoscopic Sequence 4 of 24.
Ménétrier's disease is a rare disorder characterized by
diffuse hyperplasia of the foveolar epithelium of the body
and fundus combined with hypoproteinemia resulting from
protein-losing enteropathy. Other symptoms, such as
weight loss, diarrhea, and peripheral edema, are also often
present. In rare (mostly pediatric) cases, the antrum may
be involved. In adults, onset is typically between 30 and 60
years of age, with a male-to-female ratio of 3 : 1. The
syndrome is characterized by pronounced GI protein loss
and hypoalbuminemia. Although the clinical and pathologic
features of Ménétrier's disease in children are essentially
similar to those in adults, many children have a history of
recent respiratory infection, peripheral blood eosinophilia,
and cytomegalovirus infection. Interestingly, the disease is
usually self-limited in children, generally lasting only
several weeks.
|
|
 |
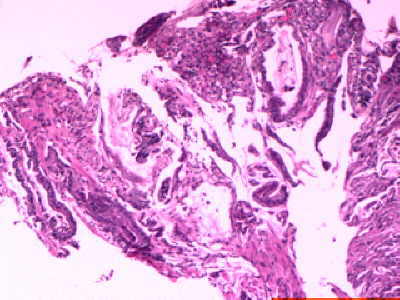
Video Endoscopic Sequence 5 of 24.
Menetrier's disease is characterised by giant hypertrophic folds that most often involve the fundus with histological features of marked foveolar hyperplasia, atrophy of glands and an increase in mucosal thickness. Additional findings include loss of enteric proteins and hypoalbuminemia, excess mucus secretion, decreased gastric acid secretion and normal or slightly elevated fasting serum gastrin astric carcinoma. The cause of the disease is unknown, although infections with Helicobacter pylori in adults and cytomegalovirus in children have been implicated. A few cases have been reported to be inherited as a dominant trait. The differential diagnosis of Menetrier's disease includes other forms of hypertrophic gastropathy such as Zollinger-Ellison syndrome, hypertrophic hypersecretory gastropathy, lymphocytic gastritis, or an infiltrating neoplasm. Spontaneous remission of the disease is rare. There is no established treatment. Reported treatments include anticholinergics, H2 receptor antagonists, tranexamic acid, corticosteroids and H. pylori eradication. Partial or total gastrectomy is generally reserved for patients with debilitating disease and for cases at risk of developing gastric cancer.
|
|
 |
Video Endoscopic Sequence 6 of 24.
|
|
 |
Video Endoscopic Sequence 7 of 24.
Although no bacteria of helicobacter pyloris were found in the fist biopsies we decided to administer treatment
This is the second endoscopy practiced two months after 21
days of treatment for Helicobacter pyloris.
|
|
 |
Video Endoscopic Sequence 8 of 24.
A gastric ulcerated fold is displayed
|
|
 |
Video Endoscopic Sequence 9 of 24. |
|
 |
Video Endoscopic Sequence 10 of 24. |
|
 |
Video Endoscopic Sequence 11 of 24. |
|
 |
Video Endoscopic Sequence 12 of 24.
The patient underwent a total gastrectomy.
|
|
 |
Video Endoscopic Sequence 13 of 24.
There has been no proven medical treatment for
Ménétrier’s disease although the patient may undergo
subtotal gastectomy if the condition is severe. The patient
would also require surveillance as there is an associated
risk of stomach cancer.
|
|
 |
Video Endoscopic Sequence 14 of 24.
In 1888, Pierre Ménétrier, a French pathologist, described
certain pathologic gastric changes, which he divided into
two anatomic groups. One group he called polyadenomes
polypeux, which are probably the equivalent of multiple
hyperplastic polyps. The other group, which he referred to
as polyadenomes en nappe, were accompanied by gastric
rugal hypertrophy; this is the group to which the term
Menetrier disease is applied.
|
|
 |
Video Endoscopic Sequence 15 of 24. |
|
 |
Video Endoscopic Sequence 16 of 24.
Ménétrier disease is listed by the Office of Rare Diseases
of the National Institutes of Health as a rare disease, a
designation that means it has a prevalence of less than 1 in
200,000 people. The hallmark of the disease is gastric
mucosal hypertrophy, which may cause the rugae to
resemble convolutions of the brain.
|
|
,
predominantly in boys (male-to-female ratio, 3:1). The
second peak occurs in adulthood, and the disease in adults
tends to progress over time. The average age at diagnosis
is 55, and men are affected more often than women.") |
Video Endoscopic Sequence 17 of 24.
The thickening of the rugae is predominantly caused by the
expansion of the epithelial cell compartment of the gastric
mucosa. Patients with Ménétrier disease most often
present with epigastric pain, hypoalbuminemia secondary t
a loss of albumin into the gastric lumen, and an increased
loss of enteric protein , which may manifest as an elevated
fecal α1-antitrypsin level. Other signs and symptoms of
Ménétrier disease include anorexia, asthenia, weight loss,
nausea, gastrointestinal bleeding, diarrhea, edema, and
vomiting. The disease has a bimodal age distribution. The
childhood form is often linked to cytomegaloviral infection
and usually resolves spontaneously. It usually occurs in
children younger than 10 years (mean age, 5.5 years),
predominantly in boys (male-to-female ratio, 3:1). The
second peak occurs in adulthood, and the disease in adults
tends to progress over time. The average age at diagnosis
is 55, and men are affected more often than women.
|
|
 |
Video Endoscopic Sequence 18 of 24.
|
|
 |
Video Endoscopic Sequence 19 of 24.
|
|
 |
Video Endoscopic Sequence 20 of 24.
|
|
 |
Video Endoscopic Sequence 21 of 24.
|
|
 |
Video Endoscopic Sequence 22 of 24.
|
|
 |
Video Endoscopic Sequence 23 of 24.
|
|
 |
Video Endoscopic Sequence 24 of 24.
|
|
|
|
|
|
|