 |
|
 |
Video Endoscopic Sequence 1 of 13.
Paraesophageal Hernia and Barrett Esophagus.
This is the case of a 63 year-old woman that has been
suffering of long-standing reflux disease.
For more endoscopic details, download the video clip by clicking on the endoscopic image. Wait to be downloaded complete then Press Alt and Enter for full screen. All endoscopic images shown in this Atlas contain video clips. We recommend seeing the video clips in full screen mode.
|
|
 |
Video Endoscopic Sequence 2 of 13.
Paraesophageal Hernia and Barrett Esophagu
Hiatal hernias may be classified into one of four types. Type I (sliding hiatal hernia) in which there is a migration of the esophago-gastric junction above the diaphragm into the thorax is the most common.
Type II is a true paraesophageal hernia in which the stomach herniates into the thorax, but the esophago-gastric junction remains fixed in its normal anatomic location below the diaphragm. Type III (mixed paraesophageal hernia) is a combination of a sliding hiatal hernia with some or all of the stomach herniating above the esophago-gastric junction.
Type IV are those hiatal hernias which include abdominal viscera and/or solid organs within the hernia sac.
Rarely, a parahiatal hernia, where gastric herniation occurs through a diaphragmatic defect separate from the hiatus, may be seen.
|
|
 |
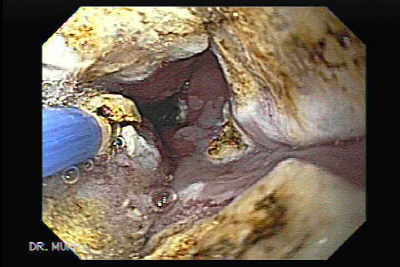
Video Endoscopic Sequence 3 of 13.
Sliding Hiatal Hernia.
The patient has also a complex hernia.
|
|
 |
Video Endoscopic Sequence 4 of 13.
Our patient also has barrett esophagus.
|
|
 |
Video Endoscopic Sequence 5 of 13.
Barrett Esophagus.
Tongues of Barrett's metaplasia.
|
|
 |
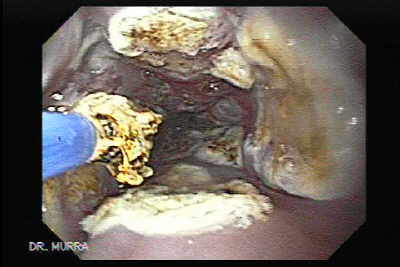
Video Endoscopic Sequence 6 of 13.
Inside the Paraesophageal hernia, there are fibers accumulated.
|
|
 |
Video Endoscopic Sequence 7 of 13.
Endoscopic Ablation of Barrett's esophagus with argon plasma coagulator.
Management of Barrett esophagus is still a clinical challenge, although the incidence of cancer appears to be low, occurring in 0.5% of patients with Barrett esophagus.
|
|
 |
Video Endoscopic Sequence 8 of 13.
Argon plasma coagulation is one of several techniques
used to ablate Barrett's esophagus.
|
|
 |
Video Endoscopic Sequence 9 of 13.
Endoscopic ablation of Barrett's esophagus using high power setting argon plasma coagulation 90 watts.
|
|
 |
Video Endoscopic Sequence 10 of 13.
Mechanical ablation includes: Endoscopic Mucosal Resection (EMR), and removing the area by biopsying it..
EMR appears to be a reasonable option to esophagectomy in patients with high grade dysplasia or adenocarcinoma limited to the mucosa It appears logical to start the evaluation of a person with Barrett’s esophagus with a suspicious lesion (polyp, nodule, erosion and so on) or an already diagnosed adenocarcinoma with endoscopic ultrasound (EUS).
This can help better define the target lesion and confirm that malignancy is limited to the mucosa. The next step would be to remove the target lesion by EMR (strip or suck methods).
After EMR has eliminated the area of invasive cancer, the remainder of the dysplastic mucosa can be managed by less invasive ablative techniques like photodynamic therapy (PDT), argon plasma coagulation (APC) or multipolar electrocoagulation (MPEC).
|
|
 |
Video Endoscopic Sequence 11 of 13.
APC is a technique that delivers controlled monopolar electrocoagulation via a stream of ionized argon gas ignited by a high voltage discharged at the tip of a specialized flexible probe.
It is a noncontact ablative method with a predetermined depth of injury (approximately 2 mm) that is most often used for coagulation of bleeding surface lesions such as arteriovenous malformations.
|
|
 |
Video Endoscopic Sequence 12 of 13.
Estatus posterior a la terapia ablativa.
APC treatment of Barrett's esophagus is simple, efficacious and safe. Reversal of Barrett's mucosa can be achieved by a few endoscopic sessions. But long term follow-up studies on many patients are necessary to establish the frequency of endoscopic surveillance on the basis of recurrence or dysplasia evolution risk, in spite of APC treatment.
|
|
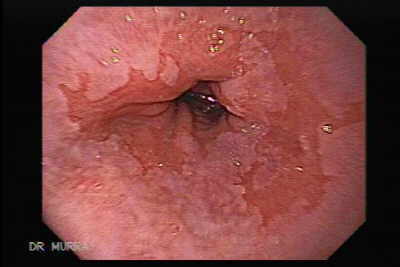 |
Video Endoscopic Sequence 13 of 13.
A follow up endoscopy was performed six months after the APC ablation.
Due to the APC ablation the tongues have been shortened,
but there is Barrett epithelium yet, a new session of APC
will be programmed.
|
|
 |
Para Esophageal Hernia.
One must see the video clip.
There is a small diverticula that can also be seen.
|
|
|
|
|
|
|